it has been quite some time since last i updated the blog... a lot has been happening here. the biggest change is that Andrew has developed cancer. the lymph nodes on his neck enlarged while i was at ACVIM and we have been crashing through the medical machine at relative speed to be able to the name 'the monster' for knowing its name will give us power over it and allow us to make a plan.
yesterday was the summative meeting with the oncologist. it went better than expected with a couple surprises.
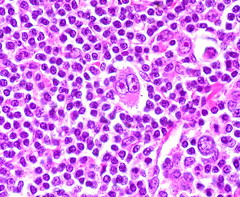
we knew going in that Andrew most likely has Hodgkins lymphoma, given his age and clinical signs. the hematopathologist was kind enough to review Andrew's slide with us and point out a number of probable Reed-Sternberg cells. we are trying to get hold of the pathologist to see if we can get digital photos of Andrew's RS cells. we would like to create prints to put up around the house, sort of like Wanted Posters! Andrew can then use his eyes to teach his immune system which cells need help dying. (cancer, after all, reflects an inability of the cell to die a normal death, eg apoptosis, due to mutation.) in the meantime, here a great photo i found on Flickr of a RS cell surrounded by visually normal lymphocytes:
there are two big things in determining treatment and prognosis. the first is determining the Stage, e.g. how far the cancer has spread. the Stages are:
Stage 1: cancer is located in a single region, usually one lymph node and the surrounding area.
Stage 2: cancer is located in two separate regions, an affected lymph node or organ and a second affected area, but both affected areas are on the same side of the diaphragm.
Stage 3: cancer has crossed the diaphragm, but remains confined to lymphatic organs.
Stage 4: the cancer has spread to one or more extralymphatic organs, such as liver, bone marrow, or lungs
there are also SubStages:
A: No clinical signs
B: Clinical signs including unexplained weight loss, night sweats or unexplained fever
based on his PET CT scan, Andrew has two foci of activity in his spleen in addition to the big dog activity in his neck and chest. he does not appear to have activity in the liver or other non-lymphatic organs. provided his bone marrow is not involved, this would make him a Stage 3. unfortunately, bone marrow activity cannot be seen on PET scan so biopsy is required to rule out marrow involvement, which the oncologist did yesterday at the end of the appointment. (surprise!) Andrew was a real trooper. my hero, as ever.
now to substage... after a detailed discussion of our sleep habits, the oncologist ruled that Andrew's only cancer-related clinical signs were night sweats were the 5 days when the nodes 'bloomed' in his neck. this is HUGE because it means that Andrew officially is a substage A (which is associated with a better outcome). YAY!
for those of you paying attention, we need one other puzzle piece to determine treatment... that is the Type of Hodgkins Lymphoma. yes - there are different types of Hodgkins. here is the list:
Nodular Sclerosing: the most common type of HL. this type is associated with deposition of secondary scar tissue in the cancer areas, which means that tissues may not return to pre-cancer size even if the cancer disappears. this is why PET scans are used over CT scans to monitor resolution of therapy - they measure activity in addition to size.
Mixed celluarity: similar to above but without scar tissue.
Lymphocyte rich: quite rare.
Lymphocyte depleted: quite bad.
Nodular lymphoctye predominant: rare. very slow growing. often responds to wimpier chemo.
Monday, Andrew had a surgical biopsy taken to determine Type. they went ahead and placed a jugular port for chemo at the same time. this is a wonderful invention that means Andrew will not have to have repeated IV catheterizations for chemo and decreases the risk of chemo extravasation.
so, the bottom line... provided the bone marrow is clean, Andrew will be classified as having Nodular Sclerosing Hodgkins, Stage 3-A. the treatment standard is ABVD given once every 2 weeks, but it will be 12 2-week cycles instead of the 3-4 cycles used for Stage 2. [we are bracing for a long six months!] on the flip, because the disease is so widespread, involved-field radiation is generally no longer in the picture. so instead of two therapy types with differing side effects, we will only be facing one but it will go much much longer.
the goal is still cure - thank the Lord for large mercies. McCachren is estimating overall 90-95% 5-year survival with 80% chance of cure with this treatment plan. (McCachren really thinks ABVD should make Andrew better, though he promises we will end up hating him first.) if this does not work, we may be looking at less fun treatment protocols (myeloablative therapy and stem cell transplant etc) but still with the end goal of Andrew and me getting old and defective together. YAY!
there are still a few tests to go. because of the potential for long-term heart and lung damage from the chemo, Andrew needs to have an echo and pulmonary function testing. also, since he is a fine, young buck, sperm banking. frustratingly, the sperm banking may delay starting chemo for a whole week. :( there is only one place in town and the woman who books appointments won't be in till Tuesday. if we can get that done in time, Andrew can get his first round of chemo Thursday the 7th. otherwise we are looking at the following week. we would obviously prefer not to wait, especially since Andrew's fatigue is worsening rather quickly and his appetite is now come and go. frustrating.
still - all in all - better news than we had dare hope!
we marvel daily at all our gifts - having one another to buoy, comfort, tease and caretake in turn; our amazing medical team who have all been great at their jobs, expedited the work-up so we could still take our trip to Glacier National Park, and have by turns been tender and funny and patient and just the right amount of chiding; our remarkable and loving circle of friends and family, who every day surprise us with new resources, 'normal' attitudes and thoughtful offers; and a wonderful God made manifest in the striking and monumental vistas of Glacier, the presence of a new bird at our feeder, the kindness of strangers, and the strength that fills us when we had been certain we were empty.
 we look forward to learning and growing throughout this amazing and harrowing adventure. we hope you will join us!
we look forward to learning and growing throughout this amazing and harrowing adventure. we hope you will join us! ps. Andrew has started a blog, for those who wish to play along at home. i know he would love your comments.
pps. for those artistically inclined (or not), we would love to fill the house with words of encouragement and love and images of all the wonders in nature that will await us when we complete this odyssey and get to embark on the next. shout at me if you need our address.


1 comment:
Good luck and I'll think of something artistic to share!
Post a Comment